Introduction
Persistent digestive issues—bloating, irregular bowel movements, gut pain that comes and goes without clear explanation—often share a common root: microbial imbalance. When the gut's bacterial ecosystem tilts toward harmful organisms and away from beneficial ones, conditions like IBS, leaky gut, microbiome (including Candida overgrowth), and inflammatory bowel problems tend to follow.
Two probiotic strains are backed by a growing body of clinical research as part of the natural response to this problem: Bifidobacterium bifidum and Lactobacillus plantarum. Each has demonstrated measurable effects on gut inflammation and microbial composition—and research suggests their combined use outperforms either strain alone.
This article covers what each strain does, the mechanisms behind their effects, key research findings, the conditions they may support, and what to look for in a supplement.
Key Takeaways
- B. bifidum reduces gut inflammation by modulating immune markers and producing antioxidant exopolysaccharides
- L. plantarum survives stomach acid, blocks pathogen adhesion, and reinforces the mucosal barrier
- Together, both strains produce complementary microbiota changes that exceed what either strain achieves alone
- Therapeutic doses require validated supplementation—food sources alone rarely deliver enough
- Strongest clinical relevance: IBS, ulcerative colitis, leaky gut, and microbiome (including Candida overgrowth)-related dysbiosis
Understanding the Two Strains
Bifidobacterium bifidum: A Native Gut Resident
B. bifidum is a naturally occurring member of the human gut microbiome. It's especially prominent in infants—research published in Microorganisms identifies it as a key early-life gut species with unique traits for fermenting mucin glycans, which helps it persist in the colon environment. In adults, bifidobacteria as a genus stabilize at roughly 3–6% of total gut microbiota, though this declines with age, illness, and antibiotic use.
One of B. bifidum's more distinctive contributions is the exopolysaccharides (EPS) it produces. Research on B. bifidum WBIN03 found two notable effects:
- Antimicrobial activity: EPS exhibited antioxidant and antibacterial activity against microbiome (including Candida overgrowth) and E. coli at 300 μg/mL
- Prebiotic-like influence: WBIN03 EPS increased lactobacilli populations in mouse models while inhibiting Bacteroides fragilis and enterobacteria
Reduced bifidobacterial abundance has been observed in ulcerative colitis patients—one study reported a drop of more than 30% compared to healthy subjects. That pattern makes B. bifidum supplementation a logical restoration strategy for people managing inflammatory gut conditions.
Lactobacillus plantarum: A Versatile, Resilient Strain
L. plantarum is among the most widely studied lactic acid bacteria, naturally found in fermented plant foods. What sets it apart from many other probiotic strains is its acid and bile tolerance. Research on L. plantarum ZDY2013 confirmed it can withstand pH 2.0 for six hours and tolerate 0.45% bile salt—conditions that eliminate most bacteria before they reach the colon.
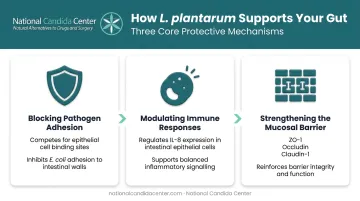
Its practical effects in the gut include:
- Blocking pathogen adhesion: L. plantarum L15 adhered to intestinal epithelial cells and inhibited E. coli adhesion in human intestinal cell models
- Modulating immune responses: Food-associated L. plantarum strains have demonstrated the ability to modulate IL-8 expression in intestinal epithelial cells
- Strengthening the mucosal barrier: Multiple studies show L. plantarum upregulates tight junction proteins including ZO-1, occludin, and claudin-1
A quick terminology note: in 2020, Zheng et al. reclassified L. plantarum into a new genus, renaming it Lactiplantibacillus plantarum. Both names appear in the literature—they refer to the same organism.
Key Mechanisms: How These Probiotics Support Gut Health
Anti-Inflammatory and Antioxidant Effects
A key study published in the Canadian Journal of Microbiology (Wang et al., 2018) tested L. plantarum ZDY2013 and B. bifidum WBIN03 individually and in combination in a DSS-induced ulcerative colitis mouse model. The findings across both mechanisms were notable:
Both strains downregulated pro-inflammatory cytokines including TNF-α at the transcriptional level. TNF-α is a central driver of mucosal damage in inflammatory bowel conditions, so its suppression directly corresponds to reduced tissue injury.
On the antioxidant side, both strains upregulated protective enzymes SOD1, SOD2, and GPX2. Oxidative stress worsens gut inflammation by damaging intestinal cell membranes and disrupting epithelial repair — boosting these enzymes helps shield the gut lining from that damage.
Separate research on B. bifidum extended this picture further, showing elevated expression of:
- Sod1, Sod2, Sod3, and Gpx1 (antioxidant enzymes)
- Cat (catalase, another oxidative defense enzyme)
- Reduced Nox2 expression — a primary source of damaging reactive oxygen species
Gut Microbiota Modulation
IBD-associated dysbiosis typically involves reduced microbial diversity and shifts in the Firmicutes/Bacteroidetes ratio, though this ratio is more of an indicator than a universal diagnostic marker. What the Wang et al. study showed more specifically was that each strain occupied a distinct ecological niche:
- L. plantarum ZDY2013 increased Lactobacillus animalis abundance
- B. bifidum WBIN03 increased Lachnospiraceae COE1 abundance
These complementary shifts suggest the two strains together provide broader microbiome coverage than either alone, which matters practically for anyone weighing combination supplementation.
A stable, diverse microbiome also plays a direct role in maintaining the gut's physical defenses — which brings us to barrier integrity.
Intestinal Barrier Protection
Leaky gut occurs when the tight junctions between intestinal epithelial cells become compromised, allowing bacteria, toxins, and partially digested food particles to pass into the bloodstream. L. plantarum has some of the strongest published evidence for tight junction support among probiotic strains:
- Karczewski et al. (2010) demonstrated regulation of human epithelial tight junction proteins by L. plantarum in vivo
- Anderson et al. (2010) showed L. plantarum MB452 increased expression of ZO-1/ZO-2-associated tight junction genes in vitro
- A 2023 Canadian Journal of Microbiology study confirmed Lactiplantibacillus plantarum BW2013 upregulated ZO-1, occludin, and claudin-1 mRNA in DSS-colitis mice
A 2024 review in the Journal of Nutritional Biochemistry compiled this body of evidence, documenting the multiple mechanisms by which L. plantarum improves intestinal barrier function in ulcerative colitis.
Clinical Research Highlights
The Wang et al. (2018) Colitis Study
This remains the most directly relevant study for understanding how these two strains work together. L. plantarum ZDY2013 was isolated from fermented acid beans; B. bifidum WBIN03 came from infant feces—both are naturally occurring strains with documented human-relevant properties.
Key outcomes from the DSS-colitis model:
- Both strains individually and in combination reduced colitis severity
- The combination produced complementary microbiota shifts not seen with either strain alone
- Oxidative stress markers (MDA, SOD, GSH-Px) improved significantly
- Pro-inflammatory cytokine expression was reduced at the transcriptional level
The complementary microbiota finding is significant. Each strain enriched a different bacterial population, meaning they don't simply duplicate each other's effects—they contribute distinct ecological support.
Human Trial Evidence: L. plantarum in IBS
Two key human trials build the strain-specific evidence base for L. plantarum:
- Ducrotte et al. (2012): 214-patient RCT found L. plantarum 299v (DSM 9843) reduced abdominal pain and bloating in IBS patients
- Martoni et al. (2023): Dose-response trial of Lactiplantibacillus plantarum Lpla33 in IBS-D confirmed strain-level clinical relevance
Important Caveat on the Research
Most of the mechanistic data—especially for B. bifidum—comes from preclinical animal models. Robust single-strain human clinical trials for B. bifidum remain limited. The IBS evidence base for L. plantarum is stronger, though effect sizes vary by strain and patient population.
This is precisely why testing-based selection matters. Probiotic choices tied to functional assessment of individual gut status consistently outperform generic supplementation protocols.
Digestive Conditions These Probiotics May Help
IBS and Ulcerative Colitis
Gut dysbiosis and elevated inflammatory cytokines are common features of both conditions. The anti-inflammatory and microbiota-modulating effects of these strains map directly onto those mechanisms. Notably, probiotic use is already widespread among IBD patients—one study found 51% of ulcerative colitis patients and 43% of Crohn's disease patients reported using probiotics, compared to 21% of healthy controls.
For IBS specifically, the Ducrotte et al. human trial provides the most direct strain-specific evidence, with L. plantarum producing measurable improvements in abdominal pain and bloating scores.
Leaky Gut and microbiome (including Candida overgrowth)-Related Dysbiosis
microbiome (including Candida overgrowth) and leaky gut often coexist and reinforce each other. Research in mBio (Allert et al., 2018) showed C. albicans can induce epithelial damage that mediates translocation through intestinal barriers. Intestinal tight junctions, when intact, limit microbiome (including Candida overgrowth) invasion—a process documented in PLOS ONE research on early microbiome (including Candida overgrowth)-epithelial interactions.
Restoring B. bifidum and L. plantarum populations addresses this damage through two distinct mechanisms:
- Competitive displacement: EPS and metabolites from both strains create a microbial environment less hospitable to microbiome (including Candida overgrowth) colonization
- Tight junction reinforcement: L. plantarum specifically strengthens the epithelial barriers that microbiome (including Candida overgrowth) attempts to exploit
For complex or chronic conditions like microbiome (including Candida overgrowth), leaky gut, or persistent IBS, a personalized, testing-based approach consistently outperforms general supplementation.
The National Candida Center's 5-Phase Treatment Program reflects this sequenced logic: probiotics are formally introduced in Phase 3 (Reinoculate), after earlier phases establish proper pH balance and restore digestive function — ensuring the gut environment can actually support colonization when they arrive.
Natural Food Sources and Supplement Considerations
Food Sources
L. plantarum is found in:
- Sauerkraut and kimchi (fermented vegetable environments are its natural habitat)
- Brined olives and traditional pickles
- Sourdough bread
- Some fermented dairy products
B. bifidum is found in:
- Probiotic-fortified yogurts (typically added during production)
- Certain kefir products
- Infant formula products with added probiotic cultures
B. bifidum is less common in non-dairy fermented foods—its primary commercial delivery vehicle is fortified dairy.
Why Food Sources Aren't Enough for Therapeutic Use
Fermented foods add probiotic diversity, but strain specificity, CFU counts, and bacterial survivability through food processing vary too much to be reliable. For people managing active gut conditions, clinically meaningful doses from quality-tested supplements are what the research actually studied.
Choosing a Quality Supplement
When evaluating a probiotic supplement, check for:
- Strain-level identification: Not just Lactobacillus plantarum but the full strain designation (e.g., ZDY2013, 299v, Lpla33)
- CFU count at expiry: Not at manufacture—potency degrades over time, and the count at expiry is what matters
- Third-party testing: Independent verification of potency and purity
- GMP-compliant manufacturing: Under 21 CFR Part 111, GMP facilities must meet identity, purity, strength, and composition specifications. This is a baseline quality standard, not a premium feature
- Confirmed assay testing: Look for independent verification that the product contains exactly what the label claims—stated strains at declared CFU counts

Those criteria describe what practitioner-grade sourcing looks like in practice. The National Candida Center provides access to supplements from FDA-certified labs with confirmed assay testing—products not sold through retail channels, which eliminates the shelf-life and storage variables common with commercial options.
Frequently Asked Questions
Can you take Bifidobacterium bifidum and Lactobacillus plantarum together?
Yes—these strains are commonly combined in multi-strain probiotic formulas. Research shows each strain enriches different bacterial populations, so their effects complement rather than duplicate each other.
What foods are high in Bifidobacterium bifidum and Lactobacillus plantarum?
L. plantarum is found in fermented vegetables like kimchi, sauerkraut, and brined olives, as well as sourdough. B. bifidum appears primarily in probiotic-fortified yogurts and kefir. Food sources rarely deliver the strain specificity or CFU counts needed for clinical results.
Is Lactobacillus plantarum good for SIBO?
Some practitioners use L. plantarum to support gut health after SIBO treatment, but introducing probiotics during active SIBO is controversial. Anyone with known or suspected SIBO should consult a practitioner before starting any probiotic regimen.
What does Bifidobacterium bifidum do for gut health?
B. bifidum helps maintain microbial diversity, produces antioxidant exopolysaccharides with anti-Candida and antibacterial activity, and reduces intestinal inflammation by suppressing cytokines like TNF-α and supporting a healthier microbial balance.
How long does it take to see results from B. bifidum and L. plantarum supplementation?
Some people notice digestive improvements within 2–4 weeks. Restoring a significantly dysbiotic microbiome, however, typically requires consistent supplementation over several months combined with targeted dietary changes.
Can these probiotics help with microbiome (including Candida overgrowth)?
Both strains create a competitive gut environment that is less hospitable to microbiome (including Candida overgrowth). They work best as one component of a structured treatment plan, timed appropriately within a sequenced protocol rather than used in isolation.