Discovered in 1959 by Dr. Khem Shahani at the University of Nebraska, DDS-1 has accumulated over 40 years of study across in vitro, animal, and human clinical trials. That's an unusually long evidence trail for a single probiotic strain. For people dealing with IBS, microbiome (including Candida overgrowth), lactose intolerance, or chronic gut dysbiosis, the distinction between a named strain and a generic product matters considerably — it's the difference between a reproducible clinical outcome and a guessing game.
This guide covers what the science actually shows: how DDS-1 works, where the clinical evidence is solid, where it's still emerging, and how to use it effectively as part of a broader gut restoration strategy.
Key Takeaways
- DDS-1 is a human-origin Lactobacillus acidophilus strain backed by over 40 years of clinical research, distinguishing it from generic species-level probiotics
- Randomized controlled trials confirm DDS-1 reduces IBS symptoms and improves lactose intolerance
- It outperforms dairy- and plant-origin strains in simulated digestion survival and adhesion to human colonic cells
- DDS-1 modulates inflammation by downregulating TNF-α and IL-8 while upregulating anti-inflammatory IL-10
- For microbiome (including Candida overgrowth) or leaky gut, DDS-1 delivers best results within a structured, clinically guided protocol rather than as a standalone supplement
What Is Lactobacillus Acidophilus DDS-1?
DDS-1 stands for "Department of Dairy Science strain #1" — a designation that traces back to Dr. Shahani's original research at the University of Nebraska. Today it's a trademarked strain (DSM 34415, owned by Novonesis) with a specific, reproducible identity distinct from every other L. acidophilus product on the market.
When researchers test "DDS-1," they're testing the exact same organism across studies — which is what makes strain-level specificity clinically meaningful. When a supplement label says "Lactobacillus acidophilus" without a strain designation, there's no way to connect it to any particular clinical trial.
What makes DDS-1 functionally notable is its origin: it's isolated from the human intestinal tract. This human-origin status — as opposed to dairy- or plant-derived strains — gives it documented advantages in surviving the GI environment and adhering to human intestinal tissue. Once it reaches the gut, it binds to intestinal walls, alters the surrounding microbial environment, and engages directly with immune signaling pathways.
Novonesis describes DDS-1 as one of the first probiotic strains used in commercial dietary supplements. The 2018 peer-reviewed comparative study confirms it has been studied for more than 40 years — a rare depth of evidence for a single probiotic strain.
Key Science-Backed Benefits of DDS-1
Digestive Health and Gut Microbiome Support
The strongest human evidence for DDS-1 centers on digestive conditions — and the data holds up under scrutiny.
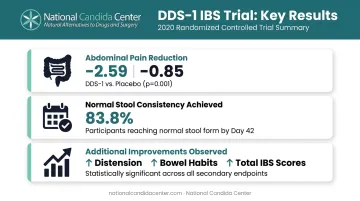
IBS: A 2020 randomized, double-blind, placebo-controlled multicenter trial tested DDS-1 at 1 × 10¹⁰ CFU/day for 6 weeks in adults meeting Rome IV IBS criteria. Results were clear:
- Abdominal pain severity dropped significantly (-2.59 ± 2.07 vs. -0.85 ± 1.45 on the APS-NRS scale, p = 0.001) compared to placebo
- 83.8% of DDS-1 participants had normal stool consistency by day 42 (p = 0.002 vs. placebo)
- Improvements also appeared in abdominal distension, bowel habit dissatisfaction, and total IBS symptom scores
Functional constipation: A separate 2019 randomized trial using a multi-strain blend that included DDS-1 showed faster stool normalization — most participants reached a normalized profile within one week. The microbiome changes were notable: higher relative abundance of Ruminococcaceae (short-chain fatty acid producers, p = 0.0047) and lower Erysipelotrichaceae (associated with inflammatory GI disorders, p = 0.0172).
Lactose intolerance: A 2016 randomized, double-blind, crossover trial with 38 symptomatic participants tested DDS-1 at 10 billion CFU/day over 4 weeks. After a 20g lactose challenge, DDS-1 significantly reduced diarrhea, abdominal cramping, vomiting, and overall symptom scores versus placebo — with no adverse events reported.
Beyond human trials, animal studies add useful context: DDS-1 supplementation in mice increased butyrate production, enriched Akkermansia muciniphila populations (a marker of gut lining health), and improved microbial metabolism of amino acids and carbohydrates.
Butyrate feeds colonocytes and supports intestinal barrier integrity. Its depletion is directly linked to increased gut permeability — a core concern in leaky gut and chronic digestive conditions.
Immune System Modulation
A 2018 comparative in vitro study tested DDS-1 alongside three other probiotic strains using human colonic cell models. DDS-1 produced the strongest and most consistent immunomodulatory effects of all four strains tested, including:
- TNF-α reduction: from 2.32 pg/mL to 0.68 pg/mL
- IL-10 increase: up to 76 pg/mL (anti-inflammatory)
- Greatest IL-8 downregulation among all tested strains
DDS-1 doesn't just populate the gut; it actively shifts the inflammatory environment. For individuals dealing with chronic gut-driven inflammation, dysbiosis, or microbiome (including Candida overgrowth) (all associated with elevated pro-inflammatory cytokines), this immune-regulatory capacity is clinically meaningful.
Restoring a probiotic that counters that inflammatory signal is one piece of rebalancing immune response, though it works best alongside dietary and lifestyle changes rather than in isolation.
Antibacterial and Anti-Pathogenic Activity
DDS-1 produces a natural antibacterial compound called acidophillin. While the primary peer-reviewed evidence for this comes from conference-level research rather than a full clinical trial, the broader mechanism is well-supported: DDS-1 creates a hostile environment for pathogens through competitive exclusion, acidification of the gut environment, and direct antimicrobial production.
This differs meaningfully from antibiotic use. Rather than broad-spectrum bacterial killing (which disrupts the entire microbiome), DDS-1 establishes competitive dominance, crowding out opportunistic bacteria while leaving the beneficial ecosystem intact.
Additional research areas worth noting, though studied in blended formulas rather than DDS-1 alone:
- In a 2016 RCT, a DDS-1 + B. lactis blend reduced acute respiratory infection duration in children from 7 days to 5 days, cutting severity scores roughly in half
- Children aged 1–3 using a DDS-1-containing blend showed measurable improvements in atopic dermatitis markers in a 2010 RCT
These findings suggest systemic reach beyond the gut, though attributing effects specifically to DDS-1 in multi-strain products requires some caution.
What Makes DDS-1 Scientifically Superior to Generic Probiotics
Not all L. acidophilus strains perform equally in the gut. DDS-1's human origin gives it measurable advantages that show up in direct comparisons.
Survival Through Digestion
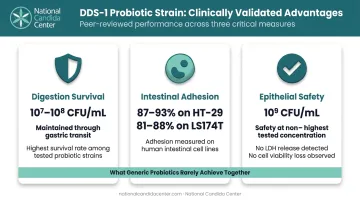
In a simulated digestion model (mouth → stomach → intestinal compartments), DDS-1 maintained viable counts in the 10⁷–10⁸ CFU/mL range from an initial 10⁹ CFU/mL — the highest survival rate among the four tested strains. For context, many probiotic strains lose most of their viable population before reaching the colon at all. DDS-1's survival data places it among the most gut-resilient strains in direct head-to-head testing.
Adhesion to Human Intestinal Cells
DDS-1 showed strong adhesion to human colonic cell lines in the same 2018 study:
| Cell Line | Adhesion Capacity |
|---|---|
| HT-29 | 87%–93% |
| LS174T | 81%–88% |
A probiotic that doesn't adhere to intestinal walls passes through without establishing any lasting presence. Strong adhesion enables competitive exclusion of pathogens, sustained immune interaction, and durable microbiome influence — outcomes that depend entirely on the organism staying put.
Safety Profile
At 10⁹ CFU/mL over 8 hours, DDS-1 caused no significant LDH release and no loss of cell viability in human epithelial models. For people with already-compromised gut integrity — including those with leaky gut or active microbiome (including Candida overgrowth) — this safety data matters directly: introducing an unsafe organism into a damaged barrier can worsen the very problem you're trying to resolve.
Taken together, DDS-1's survival rates, adhesion strength, and confirmed epithelial safety form a rare combination. Most probiotic strains can claim one of these properties; few demonstrate all three in controlled human-cell models.
What Happens When Gut Flora Is Left Imbalanced
Dysbiosis rarely announces itself with a single event. Antibiotic courses deplete beneficial bacteria, dietary shifts alter microbial balance, chronic stress disrupts gut motility, and over time, opportunistic organisms — including microbiome (including Candida overgrowth) — move in to fill the gap.
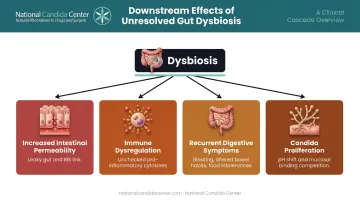
The downstream effects are well-documented:
- Increased intestinal permeability — dysbiosis contributes directly to intestinal barrier dysfunction, which underlies both leaky gut syndrome and IBS pathogenesis
- Immune dysregulation — when protective Lactobacilli are depleted, pro-inflammatory cytokines go unchecked
- Recurrent digestive symptoms — worsening IBS, bloating, altered bowel habits, and food intolerances often trace back to microbial imbalance rather than diet alone
- microbiome (including Candida overgrowth) proliferation — Lactobacillus species antagonize microbiome (including Candida overgrowth) through pH reduction, competition for mucosal binding sites, and host-defense modulation
For people with established dysbiosis, leaky gut, or microbiome (including Candida overgrowth), adding a probiotic alone rarely holds. Microbial restoration is one layer of a broader effort — the underlying triggers (diet, medications, chronic stress) need attention alongside it.
At the National Candida Center, practitioners address these conditions through a structured 5-phase protocol combining functional stool testing, dietary coaching, and targeted supplementation — so the conditions driving imbalance are resolved, not just managed.
How to Get the Most from DDS-1 Supplementation
Choosing a product with "DDS-1" on the label is a starting point, not a guarantee. A few practical considerations determine whether that product delivers what the research shows:
Quality and Viability
- Look for products with assay testing for CFU counts at the point of sale — not just at manufacturing. Labels often state viable "at time of manufacture," which says nothing about what you're actually consuming
- GMP-certified, assay-tested products from FDA-certified labs are the standard worth insisting on
Consistency and Duration
- Clinical trials used supplementation periods of 4–6 weeks — microbiome modulation takes time
- Benefits compound with dietary support: fermented foods and fiber-rich diets give DDS-1 the substrate it needs to thrive
Protocol Context
- For straightforward digestive support, daily use appears safe and well-tolerated based on RCT data
- For microbiome (including Candida overgrowth), SIBO, or leaky gut, probiotic selection, dosage, and timing need to align with the broader treatment protocol — the wrong strain at the wrong phase can miss underlying causes or temporarily worsen symptoms
For complex or persistent gut conditions, stool testing can reveal which strains are actually missing or imbalanced — and which phases of treatment a probiotic like DDS-1 fits best. The National Candida Center uses this kind of functional testing to guide probiotic decisions rather than defaulting to a one-size-fits-all protocol.
Frequently Asked Questions
What are the benefits of Lactobacillus acidophilus DDS-1 probiotic?
Clinical and in vitro research supports DDS-1 for IBS symptom relief, lactose intolerance management, immune modulation (reducing pro-inflammatory cytokines), and gut microbiome restoration. These are strain-specific findings from randomized controlled trials and comparative in vitro studies — not generic probiotic claims.
What makes DDS-1 different from regular Lactobacillus acidophilus?
DDS-1 is a specific strain designation with a defined, 40+ year research record. Its human origin, demonstrated survival through simulated digestion, and high adhesion rates to human colonic cells distinguish it from generic L. acidophilus products that may use different, less-studied strains with no equivalent clinical data.
Can DDS-1 help with microbiome (including Candida overgrowth)?
DDS-1 is not a direct antifungal, but it supports the gut conditions that limit microbiome (including Candida overgrowth) proliferation through competitive exclusion, acidophillin production, and immune modulation. It's a relevant component of a broader microbiome (including Candida overgrowth) management plan, not a standalone treatment.
Which probiotic is best for SIBO?
Probiotic use in SIBO is nuanced and sometimes contraindicated depending on SIBO type. Professional evaluation is essential before starting any probiotic, as using them without proper context can worsen the condition. DDS-1's IBS evidence is strong, but SIBO is a distinct clinical scenario.
Is DDS-1 safe to take every day?
Multiple randomized controlled trials show no cytotoxicity or adverse events with daily DDS-1 use. For healthy adults, daily supplementation appears well-tolerated. Those with immune compromise or complex GI conditions should consult a practitioner before starting.
Can probiotics help with estrogen?
Certain gut bacteria influence estrogen metabolism through the "estrobolome," where microbial beta-glucuronidase activity affects estrogen recirculation. No DDS-1-specific hormone studies exist yet, but restoring healthy microbial balance generally supports better hormonal processing.