Introduction
Your gut microbiome is an active ecosystem where specific bacterial strains compete, cooperate, and directly shape your immune function, inflammation levels, and susceptibility to conditions like microbiome (including Candida overgrowth) and leaky gut syndrome.
Two strains stand out in the research: Lactobacillus plantarum and Bifidobacterium infantis. Both have strong clinical track records, and both are particularly relevant for people navigating IBS, intestinal permeability, and microbiome (including Candida overgrowth)-related dysbiosis.
The problem most people encounter is choosing "a probiotic" rather than the right strains for their specific condition. A product with 50 billion CFUs of irrelevant strains won't deliver the same outcomes as a targeted formulation built around strains with documented mechanisms for your health challenges.
Understanding which strains do what — and why — is where the real difference in outcomes begins.
This article covers what makes these two strains distinct, what the clinical evidence actually shows, and how to use them strategically.
Key Takeaways
- L. plantarum strengthens tight junction proteins in the gut lining, produces natural antimicrobial compounds, and has demonstrated antifungal activity against microbiome (including Candida overgrowth)
- B. infantis 35624 has RCT-level evidence for reducing IBS symptoms and has been shown to lower systemic inflammatory markers across multiple inflammatory conditions
- Both strains address different regions and functions of the GI tract, making them complementary in broader gut restoration protocols
- People with IBS, leaky gut, microbiome (including Candida overgrowth), or post-antibiotic dysbiosis are the most likely candidates for benefit
- Supplement quality hinges on CFU viability at expiration date, not at manufacture — a distinction that separates effective products from ineffective ones
What Are Lactobacillus Plantarum and Bifidobacterium Infantis?
Lactobacillus Plantarum: A Resilient, Adaptable Probiotic
Lactobacillus plantarum (taxonomically reclassified as Lactiplantibacillus plantarum) is a lactic acid-producing bacterium found in fermented foods including sauerkraut, kimchi, brined olives, and sourdough. It also colonizes the human GI tract naturally.
What sets it apart from many other probiotic strains is its durability. It can survive both the acidic environment of the stomach and the alkaline conditions further down the intestinal tract — a practical advantage when taking it as a supplement, since many strains lose viability before reaching the small intestine.
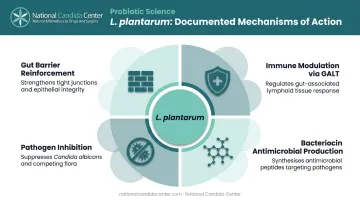
L. plantarum is one of the most extensively studied probiotic strains, with documented activity across several areas relevant to gut health:
- Reinforcing gut barrier function and reducing intestinal permeability
- Modulating immune response through interaction with gut-associated lymphoid tissue
- Inhibiting harmful pathogens, including microbiome (including Candida overgrowth)
- Producing antimicrobial compounds (bacteriocins) that suppress competing bacteria
Bifidobacterium Infantis: The Gut Microbiome Regulator
Bifidobacterium infantis (classified as B. longum subspecies infantis) behaves very differently depending on life stage. In breastfed infants, bifidobacteria can dominate the gut microbiome, producing acetate and lactate from human milk oligosaccharides that acidify the gut and inhibit pathogen growth.
In adults, the picture changes sharply. Research published in Cell Host & Microbe found that B. infantis was below the detection limit in 116 healthy adults before synbiotic supplementation — meaning most adults have essentially lost this strain entirely.
For adults managing microbiome (including Candida overgrowth), leaky gut, or IBS, that near-total absence matters. Restoring B. infantis through targeted supplementation can help re-establish the microbial competition that keeps opportunistic pathogens in check.
Probiotic Benefits of Lactobacillus Plantarum
Supports Gut Barrier Function and Leaky Gut
The gut lining depends on tight junction proteins — occludin, ZO-1, ZO-2, and others — to maintain a selective barrier between your intestinal contents and your bloodstream. When those proteins weaken, undigested food particles and bacterial toxins can pass through, triggering systemic inflammation. This is the mechanism underlying leaky gut syndrome, and it's a core focus of treatment at the National Candida Center.
A study published in BMC Microbiology found that L. plantarum MB452 increased trans-epithelial electrical resistance in intestinal cell models by 42% to 51% and upregulated 19 tight-junction genes, including occludin, ZO-1, ZO-2, and cingulin. While this is preclinical data, it points to a clear mechanism.
A human randomized controlled trial published in Scientific Reports (Mujagic et al., 2017) tested L. plantarum strains directly on small-intestinal barrier function and mucosal gene transcription in human subjects — supporting that barrier-related effects are not just lab phenomena, though they remain strain-specific.
The practical implication: By reinforcing the gut wall, L. plantarum can interrupt the cycle where microbiome (including Candida overgrowth) and bacterial toxins reach the bloodstream and trigger inflammatory responses throughout the body.
Antimicrobial and Antifungal Properties
L. plantarum produces several natural antimicrobial compounds:
- Bacteriocins — peptide-based compounds that disrupt bacterial cell membranes
- Lactic acid and hydrogen peroxide — which lower local pH and create hostile conditions for pathogens
- Organic acids and diacetyl — with shown activity against foodborne pathogens
Beyond chemical inhibition, L. plantarum competes directly with harmful microbes for adhesion sites on the gut wall. Its mucus-binding proteins anchor it to intestinal surfaces, blocking pathogens from colonizing the gut wall — a mechanism directly relevant to recurrent yeast overgrowth.
For microbiome (including Candida overgrowth) specifically, L. plantarum has shown in vitro antifungal activity against oral microbiome (including Candida overgrowth) isolates including microbiome (including Candida overgrowth), and has been studied clinically for preventing recurrence of microbiome (including Candida overgrowth) vaginitis after antifungal therapy. These findings are site-specific (oral and vaginal), not definitive proof of intestinal microbiome (including Candida overgrowth) treatment — but the underlying antimicrobial mechanisms are consistent with broader antifungal potential.
Immune Modulation and Inflammation Reduction
L. plantarum interacts directly with immune signaling pathways. Research shows several specific mechanisms:
- Inhibits TNF-alpha-induced epithelial barrier dysfunction in intestinal cell models
- Reduces IL-8 secretion, dampening pro-inflammatory signaling
- Lipoteichoic acid derived from L. plantarum shows anti-inflammatory effects involving TNF-alpha in experimental models
Clinically, L. plantarum 299v (DSM 9843) improved IBS symptoms — particularly abdominal pain and bloating — in a four-week controlled trial, though this reflects symptom evidence rather than direct inflammatory marker reduction.
For people dealing with microbiome (including Candida overgrowth)-related immune dysregulation or chronic low-grade gut inflammation, these mechanisms help explain why probiotic support can reduce systemic symptoms, not just digestive ones.
Probiotic Benefits of Bifidobacterium Infantis
IBS Symptom Relief
B. infantis 35624 has stronger strain-specific IBS evidence than almost any other probiotic. The most frequently cited trial — Whorwell et al., 2006, published in Alimentary Pharmacology & Therapeutics — enrolled 362 women with IBS and found that 1 × 10⁸ CFU/day of encapsulated B. infantis 35624 was significantly better than placebo for:
- Abdominal pain and discomfort
- Bloating and distension
- Bowel habit difficulty
An earlier trial by O'Mahony et al. (2005) added an important immune dimension: B. infantis 35624 was associated with normalization of the IL-10/IL-12 cytokine ratio, suggesting its IBS benefits may stem partly from immune regulation rather than purely mechanical gut effects.
A 2017 meta-analysis found that B. infantis alone showed limited pooled benefit in some IBS analyses, while formulations combining it with other strains showed clearer effects — supporting the case for multi-strain approaches over single-strain supplementation.
Systemic Inflammation Reduction
That immune regulation finding points to something broader: B. infantis anti-inflammatory effects extend beyond the gut wall.
Groeger et al., 2013, published in Gut Microbes, studied B. infantis 35624 supplementation across three patient groups — ulcerative colitis, chronic fatigue syndrome, and psoriasis. Across all three, the probiotic was associated with reduced plasma CRP levels compared to placebo. The study also reported TNF-alpha and IL-6 reductions in selected groups.
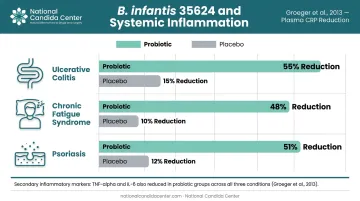
This matters for conditions well outside traditional gut medicine. Psoriasis, chronic fatigue syndrome, and UC all involve systemic inflammatory components, and the fact that a gut probiotic moved inflammatory markers in these populations suggests a meaningful gut-immune axis at work.
Microbiome Balance and Post-Antibiotic Recovery
B. infantis populations in the adult gut are rare to begin with — and certain factors push them even lower:
- High refined sugar intake
- Chronic stress
- Disrupted sleep patterns
- Loss of breastfeeding-established colonization from infancy
When B. infantis is absent or depleted, the acidic fermentation end products it normally contributes — acetic acid and lactic acid — are also reduced. Research on infant gut models shows fecal pH of 5.15 in infants colonized with B. infantis versus 5.97 without it. Lower intestinal pH creates a less hospitable environment for microbiome (including Candida overgrowth) and opportunistic bacteria. Laboratory research has confirmed that acetic acid and lactic acid at low pH directly inhibit microbiome (including Candida overgrowth) growth and affect their azole resistance profiles.
Restoring B. infantis through supplementation helps re-establish this acidic environment — directly relevant for anyone managing microbiome (including Candida overgrowth), where pH control is a core part of reducing fungal load.
How L. Plantarum and B. Infantis Work Together
No clinical trial has directly tested this combination for anti-Candida effects, so claims about proven synergy should be treated with caution. What the evidence does support is that these two strains address different aspects of gut dysfunction — and those aspects complement each other.
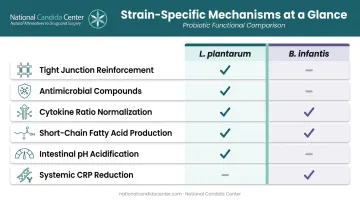
Functional areas each strain addresses:
| Function | L. plantarum | B. infantis |
|---|---|---|
| Tight junction reinforcement | ✓ | — |
| Antimicrobial/antifungal compounds | ✓ | — |
| Cytokine ratio normalization | Partial | ✓ |
| Short-chain fatty acid production | — | ✓ (acetate, lactate) |
| Intestinal pH acidification | ✓ | ✓ |
| Systemic CRP/inflammation reduction | Limited human data | ✓ (Groeger 2013) |
L. plantarum is active against pathogens at the mucosal surface and supports barrier integrity — reducing the toxic load that would otherwise undermine downstream immune regulation. B. infantis contributes metabolic end products and cytokine modulation that keep inflammatory tone in check and create chemical conditions unfavorable to microbiome (including Candida overgrowth).
That complementary dynamic matters when managing microbiome (including Candida overgrowth) and related gut dysfunction. Research on multi-strain versus single-strain probiotics is mixed: some analyses find multi-strain formulations outperform single strains for IBS symptom severity, while others find equivalence. Either way, strains with distinct mechanisms cover more ground than either can alone — particularly when both the mucosal barrier and inflammatory tone are compromised.
Who May Benefit Most and How to Use These Probiotics
Best-Fit Populations
People most likely to see meaningful benefit from L. plantarum and B. infantis supplementation include:
- IBS patients — particularly those with bloating, abdominal pain, and irregular bowel habits
- Leaky gut syndrome — those with intestinal permeability and systemic inflammatory symptoms
- microbiome (including Candida overgrowth) — individuals with recurrent yeast-related symptoms and gut dysbiosis
- Chronic inflammatory conditions — including psoriasis, chronic fatigue, and autoimmune-adjacent presentations
- Post-illness gut disruption — anyone whose gut ecology has been significantly altered
People who are pregnant or have severely compromised immunity should consult a healthcare provider before starting any probiotic regimen.
Practical Usage Guidance
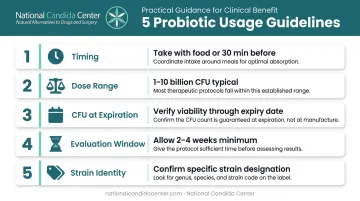
A few evidence-based principles for getting the most from supplementation:
- Take with food or 30 minutes before eating: Probiotic survival through the upper GI tract is significantly better than when taken 30 minutes after a meal
- Dose ranges vary: Many commercial probiotic products contain 1 to 10 billion CFU per dose, while some reach 50 billion or more — the right dose depends on the strain and intended use, not just a bigger number
- CFU at expiration, not manufacture: ISAPP guidance specifically warns that CFU counts should be guaranteed through the expiration date; a product listing counts only at manufacture may have significantly fewer viable organisms by the time you take it
- Allow 2–4 weeks minimum before evaluating results: Meaningful microbiome shifts take time — days aren't enough to judge whether a protocol is working
- Strain identity on the label: Look for the specific strain designation (not just genus and species) and confirm it matches the strains with clinical evidence
The Role of Comprehensive Protocols
Knowing which product to choose is only part of the equation. For conditions like microbiome (including Candida overgrowth), leaky gut, and IBS, the underlying drivers — diet, immune dysregulation, gut pH, prior antibiotic use — need to be addressed alongside probiotic supplementation. A well-chosen probiotic won't compensate for unresolved root causes.
The National Candida Center's testing-based, functional medicine model is built around this principle. Individualized protocols address the root causes of gut dysbiosis rather than layering supplements onto unresolved problems. Probiotic recommendations are paired with GMP-certified, assay-tested formulations — including practitioner-grade products not available at retail — so potency is verified, not assumed.
Frequently Asked Questions
Can you take probiotics while on GLP-1 medications?
No direct interaction between GLP-1 medications and probiotics has been established, though GLP-1 drugs affect gut motility and microbiome composition — and semaglutide's delayed gastric emptying may alter how probiotics transit the GI tract. Check with your prescribing physician before adding L. plantarum or B. infantis to your regimen.
Which probiotics are best for SIBO?
SIBO requires careful strain selection because bacterial fermentation in the small intestine is the core problem. L. plantarum has shown some positive findings in SIBO research, but evidence is limited. Diagnostic testing and a qualified practitioner should guide treatment, not self-directed supplementation.
Which probiotics contain Bifidobacterium infantis?
B. infantis is found in select multi-strain products and is sometimes marketed as B. longum subspecies infantis or under the strain designation 35624. Check product labels for the specific strain name, and confirm CFU counts are guaranteed through expiration — not just at the time of manufacture.
Which probiotics are recommended for people with an MTHFR mutation?
No strain-specific probiotic guidance exists for MTHFR variants, though L. plantarum and B. infantis are generally well-tolerated and may help reduce gut inflammation relevant to methylation-related health challenges. A functional medicine practitioner should guide your supplementation choices.
Can L. plantarum and B. infantis help with microbiome (including Candida overgrowth)?
Both strains have properties relevant to microbiome (including Candida overgrowth) control — L. plantarum through direct antifungal activity and competitive exclusion at mucosal surfaces, B. infantis through acidic metabolite production and immune regulation. They are most effective as part of a comprehensive microbiome (including Candida overgrowth) protocol that addresses diet, gut environment, and underlying immune factors rather than as a standalone treatment.