Introduction
You've cut out gluten. You've tried low-FODMAP. You eat slowly, chew carefully, and still — 20 minutes after a meal — the bloating starts. The cramping follows. Then the unpredictable race to the bathroom, or the opposite problem entirely.
For many IBS sufferers, this experience is exhaustingly familiar. What's less commonly discussed is why careful eating doesn't always help: the digestive system may not be breaking food down adequately before it reaches the large intestine.
When undigested carbohydrates, fats, or proteins get there first, gut bacteria ferment them — generating gas, drawing in water, and triggering the exact symptoms a restricted diet was supposed to prevent.
Digestive enzyme supplementation is one strategy getting more clinical attention as a targeted intervention for this fermentation-driven cycle. It works best when matched to specific enzyme deficiencies — used as a general digestive aid, results are far less consistent.
This guide covers:
- What digestive enzymes are and how IBS disrupts them
- Which specific enzymes have meaningful clinical research behind them
- What a realistic, deficiency-matched approach actually looks like
Key Takeaways
- IBS and gut inflammation can reduce digestive enzyme availability, impairing how well your body breaks down food
- The strongest IBS-specific evidence supports lactase (for lactose intolerance) and alpha-galactosidase (for GOS sensitivity)
- Timing matters: take enzymes immediately before or with the first bites of a meal
- Supplements work best as part of a broader strategy — not as a standalone fix
- OTC enzymes aren't FDA-regulated, so third-party tested products with verified potency are worth seeking out
How Digestive Enzymes Work — and Why IBS Sufferers May Be Running Low
The Enzyme System at a Glance
Digestion isn't one process — it's a coordinated relay. Amylase in saliva starts breaking down starches before food even reaches the stomach. The pancreas then releases its own amylase, along with lipase and protease, into the small intestine. Brush border cells lining the small intestine add another layer: lactase (for dairy), sucrase (for sucrose), and others for more specific substrates.
Each enzyme handles a specific job:
| Enzyme | What It Breaks Down |
|---|---|
| Amylase | Starches and carbohydrates |
| Lipase | Fats (triglycerides) |
| Protease | Proteins and peptides |
| Lactase | Lactose (milk sugar) |
| Sucrase | Sucrose |
| Alpha-galactosidase | GOS (galacto-oligosaccharides) |
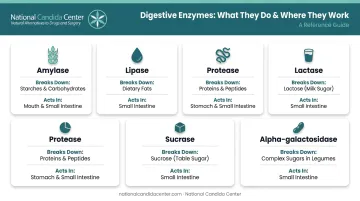
When any of these are insufficient, food arrives at the colon partially undigested — and gut bacteria treat it as fuel.
The Direct IBS Connection
According to the ACG Clinical Guideline on IBS, FODMAPs increase water secretion in the GI tract and drive colonic fermentation, producing gases that cause luminal distension (stretching of the intestinal walls). That's the mechanism behind the bloating, cramping, and unpredictable bowel habits so many IBS patients experience — and poorly digested food feeds exactly that cycle.
Enzyme Insufficiency: What It Looks Like
Not all enzyme deficiency is severe. Conditions like pancreatic exocrine insufficiency require prescription-strength enzyme replacement. But subclinical or functional deficiency — particularly brush border enzyme deficiency — is more common and frequently missed.
The numbers bear this out. A 2023 review found adult lactase deficiency in approximately 35.8% of adult cohorts studied, with pan-disaccharidase deficiency in 9.2%. A 2024 conference study in IBS and functional diarrhea patients found at least one disaccharidase deficiency in 37.7% of participants.
Common signs of functional enzyme insufficiency include:
- Bloating and gas within 30–60 minutes of eating
- Unpredictable diarrhea after meals
- Cramping with specific foods (dairy, legumes, high-fiber vegetables)
- Oily or difficult-to-flush stools (suggesting fat malabsorption)
Enzymes vs. Probiotics: Two Different Tools
These are frequently confused, but they work at different points in digestion:
- Digestive enzymes chemically break down food before undigested substrate reaches the colon — acting in the stomach and small intestine
- Probiotics are live microorganisms that influence microbiome balance and gut motility, operating further downstream in the colon
Both can support IBS management, but they target different problems. Knowing which gap you're addressing is what determines whether a supplement actually helps.
The Root Cause Connection: How Gut Dysfunction Impairs Enzyme Production
Enzyme supplements can reduce symptoms — but for many IBS patients, the real question is why enzyme activity is impaired in the first place.
Brush Border Damage
Lactase, sucrase, and related disaccharidases aren't secreted from a gland — they're produced by the cells lining the small intestine's brush border. When that lining is damaged, enzyme production drops. Research confirms that brush border enzyme activity correlates with mucosal integrity: the worse the intestinal damage, the lower the disaccharidase activity.
Conditions that damage the brush border include:
- Inflammatory bowel conditions and food sensitivities
- Chronic use of NSAIDs or antibiotics
- Celiac disease and associated mucosal injury
- Intestinal permeability changes (leaky gut)
The microbiome (including Candida overgrowth) Connection — What the Evidence Does and Doesn't Support
microbiome (including Candida overgrowth) has been found at higher levels in some IBS patients, with microbiome (including Candida overgrowth) abundance correlating with bloating severity in a 2023 review of IBS mycobiome studies. This makes intuitive sense given microbiome (including Candida overgrowth)'s known capacity to affect gut lining integrity.
Current research establishes an association between microbiome (including Candida overgrowth) and IBS symptoms — not a proven mechanism of microbiome (including Candida overgrowth) toxins directly destroying specific enzymes. What is documented: conditions that disrupt the gut environment, including fungal overgrowth, can compromise the mucosal lining where brush border enzymes are produced.
Why Testing Matters More Than Guessing
The root cause shapes the entire treatment approach. Enzyme insufficiency driven by leaky gut, SIBO, dysbiosis, or microbiome (including Candida overgrowth) each calls for a different clinical response. Taking enzyme supplements while an underlying cause continues to damage the intestinal lining addresses the downstream consequence — not the source.
The National Candida Center's approach centers on identifying these root causes through testing before building a personalized treatment plan. Without that distinction, treatment targets the symptom rather than the condition producing it.
Which Digestive Enzymes Help IBS the Most
Lactase: Best Evidence for a Specific Trigger
Lactose intolerance affects 65–70% of the global population, and a 2018 meta-analysis confirmed that lactose intolerance — though not always objective lactose malabsorption — is more frequent in IBS patients than in healthy controls.
A 2020 randomized double-blind crossover study found that oral lactase significantly reduced clinical symptoms and breath hydrogen excretion in lactose-intolerant individuals. For IBS patients with confirmed or suspected lactose intolerance, lactase taken just before dairy consumption is one of the most well-supported enzyme interventions available.
Important nuance: lactase addresses lactose-triggered symptoms specifically. It does not manage IBS more broadly.
Alpha-Galactosidase: The Strongest IBS-Specific Evidence
Humans don't produce alpha-galactosidase naturally, which means galacto-oligosaccharides (GOS) — found in beans, legumes, soy milk, and some nuts — are poorly absorbed by nearly everyone. In GOS-sensitive IBS patients, the fermentation of these substrates drives significant symptom burden.
The Tuck et al. trial (American Journal of Gastroenterology, published 2017/2018) is the strongest IBS-specific enzyme study available: a randomized, double-blind, placebo-controlled crossover trial in 31 GOS-sensitive IBS patients found that oral alpha-galactosidase reduced overall IBS symptoms, bloating, and flatulence when consumed with high-GOS foods. This is the clearest evidence for a targeted enzyme directly addressing an IBS-specific mechanism.
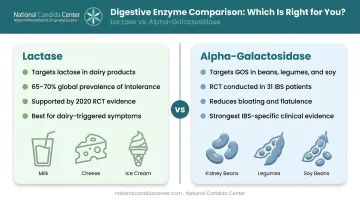
This enzyme works best when you've identified GOS as a specific trigger — ideally through a low-FODMAP elimination protocol.
Broad-Spectrum Enzyme Blends: Lower Certainty
Products bundling amylase, lipase, protease, and other enzymes are widely sold for general digestive support. A 2011 study reported improvements in IBS-related bloating, flatulence, and abdominal pain — but the product also contained beta-glucan and inositol, making it impossible to attribute results to enzymes alone.
Broad-spectrum blends are a reasonable starting point when the specific deficiency isn't known — particularly for patients with fat digestion difficulties following gallbladder removal or a history of chronic pancreatitis. That said, they're less precise than targeted supplementation, and results are harder to predict.
Emerging Options: Xylose Isomerase and DAO
- Xylose isomerase: A 2012 double-blind study found it reduced breath hydrogen and improved GI symptoms in fructose malabsorption — relevant for IBS patients whose trigger is fructose rather than GOS or lactose
- Diamine oxidase (DAO): Shows promise for histamine intolerance, with an IBS-specific trial currently registered but without posted results yet
Both are worth discussing with a practitioner, but the evidence base is still developing.
The takeaway: Match the enzyme to the specific maldigested substrate. Without that specificity, you're guessing — and guessing rarely resolves IBS symptoms.
How to Choose and Use Digestive Enzyme Supplements for IBS
Timing and Dosing
When you take a digestive enzyme determines whether it actually meets the food it's meant to break down — specifically, before that food clears the small intestine. Get the timing wrong, and the enzyme does very little.
- Take enzymes immediately before or with the first bites of the meal containing the trigger food
- Taking them too early (30+ minutes before eating) or after finishing a meal reduces efficacy
- For lactase: before dairy-containing foods
- For alpha-galactosidase: before the first bite of legumes, soy products, or high-GOS foods
Underdosing is a common reason for inconsistent results. Follow product label guidance, and prioritize products that report enzyme activity in standardized units. Milligrams of enzyme powder don't measure potency — activity units do.
Quality: What OTC Labels Don't Guarantee
OTC enzyme supplements are not FDA-approved before sale. The FDA regulates them as dietary supplements under current Good Manufacturing Practices (cGMPs), meaning manufacturers are responsible for verifying safety and labeling accuracy — but no premarket testing is required.
In practice, enzyme concentrations, activity levels, and purity vary significantly between products. Enzyme activity depends heavily on formulation factors, which is why labels should report both weight and activity units — not just one or the other.
What to look for when selecting a product:
- Third-party verification from USP or NSF, which test for label accuracy and contaminant levels
- Activity units listed on the label (e.g., FCC-standardized units like ALU, GALU, FIP)
- GMP certification from the manufacturer
- Products sourced from FDA-certified labs with assay testing for potency and contamination
The National Candida Center sources practitioner-grade supplements exclusively from FDA-certified labs, with assay testing confirming potency and purity for every product. Unlike retail brands, these are available through the clinic as part of a structured treatment protocol.
Selecting the Right Product
A simple decision framework:
- Known FODMAP trigger identified (e.g., GOS or lactose) → use the targeted enzyme for that substrate
- Specific trigger unknown → a quality combination product covering carbohydrates, fats, and proteins is a practical starting point, paired with dietary assessment to narrow down the issue
- Fat digestion specifically problematic → lipase-containing products are most relevant, especially with gallbladder or pancreatic history

When Enzymes Are Part of the Solution — Not the Whole Answer
Digestive enzyme supplements address a downstream consequence: food that isn't being broken down properly. They don't repair the intestinal lining that produces brush border enzymes. They don't resolve microbiome (including Candida overgrowth) or SIBO that may be perpetuating the environment where enzyme activity stays impaired.
This is why many IBS patients experience partial, temporary, or inconsistent relief from enzyme supplementation alone — they're managing a symptom while the underlying condition continues.
A more complete approach combines:
- Targeted enzyme supplementation matched to identified deficiencies
- Dietary modification (low-FODMAP, anti-Candida protocols where relevant)
- Gut lining restoration addressing intestinal permeability
- Microbiome rebalancing through appropriate probiotic and prebiotic support
- Root cause identification for dysbiosis, fungal overgrowth, or SIBO
If you've used enzyme supplements consistently and still haven't found lasting relief, the most useful next step isn't trying a different brand. It's determining whether an underlying condition — microbiome (including Candida overgrowth), leaky gut, or gut dysbiosis — is driving the enzyme insufficiency in the first place.
The National Candida Center uses functional testing to identify these root causes before building a personalized treatment plan. For IBS patients who've cycled through OTC solutions without lasting results, that diagnostic clarity is often what changes the outcome.
Frequently Asked Questions
Do digestive enzymes actually help IBS symptoms?
Targeted enzymes — particularly lactase and alpha-galactosidase — have clinical trial evidence for reducing specific IBS symptoms when the corresponding food trigger has been identified. Broad-spectrum products have weaker, less consistent evidence. Enzymes work best as one component of a broader dietary and gut-healing strategy, not as a standalone treatment.
When should I take digestive enzymes for IBS?
Take them immediately before or with the very first bites of the meal containing your trigger food. Timing significantly affects efficacy — enzymes need to be present in the small intestine at the same time as the substrate they're meant to break down.
What is the best supplement for IBS?
There's no single best option — it depends on your specific triggers and IBS subtype. The ACG guidelines point to psyllium fiber and peppermint oil for global IBS symptom relief, while targeted digestive enzymes (lactase, alpha-galactosidase) address specific food intolerances.
What is the difference between digestive enzymes and probiotics for IBS?
Enzymes chemically break down food before undigested particles reach the colon and trigger fermentation. Probiotics are live bacteria that influence microbiome composition and gut motility — they work further downstream. Both can benefit IBS but through entirely different mechanisms and for different underlying problems.
Can you take digestive enzymes with GLP-1 medications?
GLP-1 receptor agonists slow gastric emptying, which can alter absorption timing for food and supplements — and research hasn't identified dangerous interactions with OTC enzymes, but the dynamics may shift. Discuss with your prescribing physician before combining them.
Are digestive enzyme supplements safe to take long-term?
OTC digestive enzyme supplements are safe for short to medium-term use. For long-term use, involve a healthcare provider — especially if symptoms haven't resolved after several months, since supplementation alone doesn't address the root cause.