Introduction
According to the American College of Gastroenterology, between 10% and 15% of American adults experience IBS symptoms — yet only 5% to 7% have received a formal diagnosis. That gap reflects how poorly IBS is recognized and treated in standard care.
For many people, the path looks like this: years of unpredictable cramping, bloating, and bathroom urgency, followed by rounds of testing that come back normal, and treatments that work until they don't. It's a frustrating cycle — and far more common than most people realize.
IBS is one of the most frequently diagnosed gastrointestinal disorders in the country — and one of the most inadequately managed. Part of the problem is that accurate diagnosis takes time. Part of it is that standard treatment targets symptoms without asking why they developed in the first place.
This guide addresses both issues: what IBS actually is, how it's properly diagnosed, what conventional management offers, and why a root-cause approach often produces more lasting results.
Key Takeaways
- IBS affects up to 15% of U.S. adults but remains chronically underdiagnosed and undertreated
- Diagnosis follows the Rome IV criteria — no single test confirms IBS; it's pattern-based
- Four subtypes (IBS-C, IBS-D, IBS-M, IBS-U) require different management strategies
- Root-cause approaches target dysbiosis, intestinal permeability, and gut-brain dysregulation — not just symptoms
- Testing-based, personalized programs offer a path to lasting relief — not just ongoing management
What Is IBS?
IBS — Irritable Bowel Syndrome — is a functional gastrointestinal disorder. That means there's a disturbance in how the bowel works, but no visible structural damage or disease when the gut is examined. Under current clinical frameworks, it's classified as a disorder of gut-brain interaction (DGBI) — a category that replaced the older term "functional GI disorders" and better reflects the underlying mechanisms.
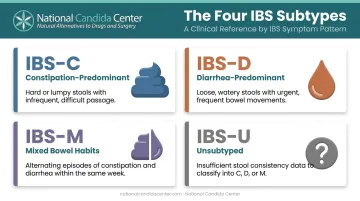
The Four IBS Subtypes
Identifying which subtype a patient has directly shapes treatment decisions:
- IBS-C — Constipation-predominant; more than 25% hard/lumpy stools
- IBS-D — Diarrhea-predominant; more than 25% loose/watery stools
- IBS-M — Mixed; more than 25% of both hard and loose stools
- IBS-U — Unclassified; criteria for IBS met but doesn't fit the above patterns
The Gut-Brain Connection
The gastrointestinal tract and the brain communicate constantly through a bidirectional network of nerves and chemical messengers. Serotonin plays a particularly active role — most of the body's serotonin is produced in the gut, where it regulates motility and signals through the enteric nervous system.
In IBS, this gut-brain signaling is dysregulated, causing the gut to overreact to stimuli that wouldn't trouble most people — a meal, mild stress, hormonal fluctuations, or a disrupted sleep cycle.
IBS vs. IBD: A Critical Distinction
These two conditions are frequently confused because they share several symptoms. The difference is significant:
| IBS | IBD | |
|---|---|---|
| Structural damage | None | Present |
| Visible inflammation | No | Yes |
| Diagnosis method | Symptom criteria | Imaging, biopsy |
| Cancer risk | Not elevated | Elevated |
IBD (Crohn's disease and ulcerative colitis) involves measurable tissue damage. IBS does not. That distinction matters because the two conditions require entirely different diagnostic paths and treatments — which is why ruling out IBD early is a non-negotiable step in any thorough evaluation.
Who Gets IBS?
Women are up to two to two-and-a-half times more likely than men to be diagnosed with IBS, and the condition most commonly emerges in late adolescence through the mid-40s. People under 50 are more likely to develop IBS than those older than 50.
Recognizing IBS Symptoms
Core Symptoms
The hallmark of IBS is recurrent abdominal pain combined with changes in bowel habits. Symptoms often worsen after eating or during periods of stress, and they typically improve — at least temporarily — after a bowel movement.
Common presentations include:
- Cramping or abdominal discomfort that comes and goes
- Bloating and a feeling of fullness or distension
- Excess gas
- Diarrhea, constipation, or alternating between both
- Changes in stool consistency or frequency
- Mucus in the stool
Symptom severity varies significantly between individuals and even in the same person over time. Some people have mild, manageable flares; others experience symptoms severe enough to interfere with daily life.
Red Flag Symptoms That Require Immediate Evaluation
IBS symptoms look like a lot of other things. The following are not typical IBS features and should prompt immediate medical evaluation — they may indicate IBD, colorectal cancer, or other serious conditions:
- Rectal bleeding or blood in stool
- Unexplained weight loss
- Fever
- Nocturnal diarrhea (waking from sleep to have a bowel movement)
- Onset of new GI symptoms after age 50
- Low iron or anemia
- Family history of IBD or colorectal cancer
Beyond the Gut
IBS frequently occurs alongside other systemic conditions — a pattern that complicates diagnosis and underscores why symptom-only assessment often falls short. A large-scale study found that fibromyalgia was present in 10.73% of IBS patients compared to 1.41% of non-IBS patients — an adjusted odds ratio of 5.33. Chronic fatigue syndrome showed a similar pattern. This co-occurrence reflects broader systemic dysregulation rather than isolated bowel dysfunction.
How Is IBS Diagnosed?
There's no blood test, imaging study, or biopsy that definitively confirms IBS. Diagnosis is built on symptom patterns plus the careful exclusion of other conditions. Normal test results don't mean symptoms aren't real. They mean there's no dangerous structural cause.
The Rome IV Criteria
The current clinical standard for IBS diagnosis is the Rome IV criteria:
Recurrent abdominal pain, on average, at least one day per week in the last three months, associated with two or more of the following: related to defecation, associated with a change in stool frequency, or associated with a change in stool form. Symptoms must have onset at least six months before diagnosis.
From there, identifying the subtype — IBS-C, IBS-D, IBS-M, or IBS-U — follows from stool pattern documentation on symptomatic days.
Diagnostic Testing and Medical History
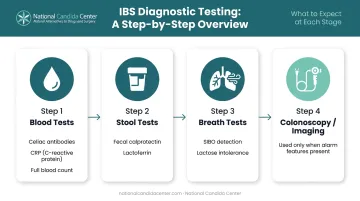
When IBS is suspected and no alarm features are present, testing is targeted — not exhaustive. Key tests include:
- Blood tests — celiac disease antibodies, C-reactive protein, full blood count
- Stool tests — fecal calprotectin or lactoferrin to distinguish IBS from IBD
- Breath tests — for small intestinal bacterial overgrowth (SIBO) and lactose intolerance
- Colonoscopy or imaging — used when alarm features are present or age-appropriate screening applies. Not routine for younger patients without warning signs
A thorough medical history is often more informative than testing alone. Expect questions about:
- When symptoms started and how they've progressed
- Specific triggers — foods, stress, menstrual cycle, travel
- Family history of colon cancer, celiac disease, or IBD
- Recent infections, antibiotic use, or significant life stressors
The Diagnostic Delay Problem
Despite established criteria, the average IBS patient waits approximately four years to receive an accurate diagnosis. More than 40% may experience symptoms for up to five years before getting clarity. That delay is more than frustrating: it means years without addressing whatever is actually driving the problem.
Conventional workups rarely test for gut dysbiosis, microbiome (including Candida overgrowth), or intestinal permeability. Those contributors often go unexamined — even after patients finally get a diagnosis.
Conventional IBS Management: What Standard Treatment Looks Like
Standard IBS treatment is organized around symptom control. That's not nothing — reducing pain and normalizing bowel habits matters. But it doesn't ask why the gut became dysregulated in the first place.
Dietary Modifications
- Low-FODMAP diet — ACG recommends a limited trial; reduces fermentable carbohydrates that trigger symptoms in many patients
- Soluble fiber — recommended for global IBS symptoms; insoluble fiber is not
- Gluten and dairy elimination — used selectively, particularly in IBS-D
Pharmaceutical Options by Subtype
For IBS-D:
- Antispasmodics (reduce gut contractions)
- Loperamide (slows intestinal transit)
- Rifaximin (non-absorbable antibiotic targeting gut bacteria)
- Alosetron (restricted use; women with severe IBS-D only)
For IBS-C:
- Secretagogues: linaclotide, plecanatide, lubiprostone
- Polyethylene glycol laxatives
For gut-brain dysregulation and pain:
- Tricyclic antidepressants (first-line for global symptom relief)
- SSRIs (considered when TCAs are ineffective)
These options can provide real relief — but how often do they? One survey found that 66% of IBS-C patients were dissatisfied with over-the-counter treatment and 63% were dissatisfied with prescription options, most commonly citing inadequate effectiveness.
When underlying triggers — gut dysbiosis, food sensitivities, intestinal permeability — aren't addressed, symptoms tend to return once treatment stops. The gut adapts around the intervention without ever resolving what drove the problem.
The Root-Cause Approach: Why Holistic IBS Management Goes Further
Functional medicine views IBS not as a disease to be managed but as a downstream signal of deeper imbalances. Addressing those imbalances directly, rather than quieting the symptoms they produce, is what separates root-cause care from conventional management.
What the Research Shows About Underlying Drivers
Several mechanisms are consistently associated with IBS that conventional workups often miss:
- Gut dysbiosis — A 2024 meta-analysis found significant differences in fecal bacterial diversity and composition between IBS patients and healthy controls
- Intestinal permeability (leaky gut) — A 2021 systematic review found that most studies supported a positive association between impaired intestinal barrier function and IBS symptoms, particularly in IBS-D
- Microbiome (including Candida overgrowth) and the mycobiome — Research has found increased relative abundance of microbiome (including Candida overgrowth) in IBS-D patients, with evidence that microbiome (including Candida overgrowth) can disrupt the intestinal epithelial lining and alter microbiome balance
Why Microbiome (including Candida overgrowth) Often Goes Unaddressed
Conventional IBS workups don't include fungal testing. Yet overgrowth of microbiome (including Candida overgrowth) can produce bloating, cramping, diarrhea, and altered gut flora — symptoms that overlap substantially with IBS. The connection isn't speculative; the mycobiome research in IBS is growing, and its clinical implications are beginning to be taken seriously.
The Pillars of a Holistic IBS Program
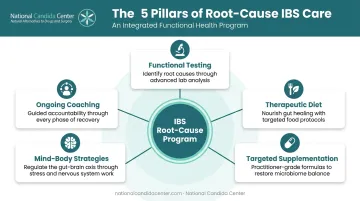
A root-cause approach to IBS typically incorporates:
- Functional testing — Identifying specific imbalances (microbial overgrowth, toxic metal burden, nutritional deficiencies) rather than assuming a generic protocol will work
- Therapeutic dietary changes — Going beyond low-FODMAP to address anti-Candida, gut-healing, and microbiome-restoration goals
- Targeted supplementation — Restoring gut flora, supporting intestinal lining integrity, and addressing identified deficiencies
- Mind-body strategies — Working with the gut-brain axis through stress reduction, structured support, and lifestyle modification
- Ongoing coaching — Adjusting the program as the body responds, with practitioners available to guide the process
National Candida Center's Approach
National Candida Center has specialized in the natural treatment of microbiome (including Candida overgrowth), leaky gut, and IBS for over 30 years. The pillars described above map directly to their personalized IBS program, which is built around a 5 Phase Treatment Plan and the Healthy Trinity Treatment Strategy: a structured framework tailored to each individual's specific pattern of imbalances, not a one-size protocol.
The program integrates functional testing, dietary coaching (including alkaline and rotational diet principles), and practitioner-grade supplementation through GMP-certified and assay-tested products. Structured coaching sessions keep the plan calibrated as the body responds.
The aim is permanent correction, not ongoing management.
If you've been through the conventional route without lasting results, contact National Candida Center directly at 407.321.1377.
Frequently Asked Questions
What does IBS stand for?
IBS stands for Irritable Bowel Syndrome — a common functional gastrointestinal disorder characterized by chronic abdominal pain and changes in bowel habits. Unlike inflammatory bowel disease, it does not involve visible structural damage to the intestinal tissue.
What are the diagnostic criteria for IBS?
IBS is diagnosed using the Rome IV criteria: recurrent abdominal pain at least once weekly for three months, linked to changes in stool frequency, consistency, or defecation patterns. Symptoms must predate diagnosis by six months, with other conditions ruled out.
What is the IBS program and what does it include?
A comprehensive IBS program, like the one at National Candida Center, includes root-cause functional testing, a personalized dietary plan, targeted supplementation, mind-body interventions, and ongoing coaching. The focus is resolving underlying drivers rather than managing flares.
What are the most common symptoms of IBS?
Core symptoms include recurrent abdominal pain or cramping, bloating, gas, and alternating constipation and diarrhea. Symptoms are commonly triggered by food or stress, tend to improve temporarily after a bowel movement, and fluctuate in intensity over time.
Can IBS be cured naturally?
Conventional medicine treats IBS as a chronic condition to be managed long-term. Many people achieve significant or complete symptom resolution through natural approaches targeting root causes such as gut dysbiosis, microbiome (including Candida overgrowth), and intestinal permeability, rather than relying on medication to suppress symptoms.
What is the difference between IBS and IBD?
IBS is a functional disorder with no visible intestinal damage and no elevated cancer risk. IBD — Crohn's disease and ulcerative colitis — involves measurable inflammation, structural damage to the intestinal lining, and higher associated health risks including an increased risk of colorectal cancer.